
No products in the cart.

Dichloropane crystal rocks
€10.95
The most extensively studied effect of dichloropane on the central nervous system is the blockade of the serotonin, dopamine, and norepinephrine transporter. This substance acts as a triple reuptake inhibitor and prevents monoamine neurotransmitters from being recycled, causing excessive amounts to build up in the synapse, or junction between neurons. The result is an enhanced and prolonged post-synaptic effect of monoaminergic signaling at receptors on the receiving neuron. It is this sudden flood of neurotransmitters in the synapses of various brain regions that is thought to cause dichloropane’s effects.
Compared to cocaine, dichloropane has a higher relative affinity for both the serotonin and norepinephrine transporters over the dopamine transporter, which is in part suspected to be responsible for the differences in its subjective effects.
Purity: 98.5%
| 1 Gram | €10.95 |
| 3 Grams | €27.95 |
| 5 Grams | €39.95 |
| 10 Grams | €74.95 |
| 25 Grams | €159.95 |
Dichloropane crystal rocks – More information
Dichloropane (also known as RTI-111 or O-401) is a novel stimulant substance of the phenyltropane class. Its effects include stimulation, thought acceleration, appetite suppression and euphoria.
It is structurally related to cocaine and shares many of its effects, although it notably lacks its local anesthetic properties.
Dichloropane has been shown to have a slower onset and longer duration of action compared to cocaine in animal studies. Anecdotal reports characterize it as having the basic stimulant qualities of cocaine but without as much euphoria, more protracted comedown, and less general enjoyability.
Dichloropane first appeared on the research chemical market around 2010. It is among to the first cocaine analog to be made available (in limited quantities) on the online research chemical market.
Very little is known about the pharmacology, metabolism, and toxicity of dichloropane. It is highly advised to use harm reduction practices if using this substance.
clinical data
| Common names | Dichloropane, RTI-111 |
| Substitutive name | (−)-2β-Carbomethoxy-3β-(3,4-dichlorophenyl)tropane |
| Systematic name | Methyl (2S,3S)-3-(3,4-dichlorophenyl)-8-methyl-8-azabicyclo[3.2.1]octane-2-carboxylate |
| Psychoactive class | Stimulant |
| Chemical class | Phenyltropane |
Dichloropane dosage table
| Threshold | 3 mg |
| Light | 10 – 20 mg |
| Common | 20 – 40 mg |
| Strong | 40 – 60 mg |
| Heavy | 60 mg + |
Dichloropane effect progress
| Total | 2 – 4 hours |
| Offset | 60 – 90 minutes |
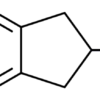
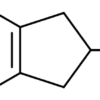
Chemistry
Dichloropane is a derivative of 3-phenyltropane. Methylecgonidine as the direct precursor to this compound. It is produced as a hydrochloride salt in its powdered form.
Dichloropane is structurally similar to cocaine, atropine and hyoscine, as it contains a tropane ring. The tropane ring of RTI-11 is substituted with a carbomethoxy group, also found in cocaine. RTI-111 differs from cocaine by its other addition, a dichlorinated phenyl ring. The phenyl ring of RTI-111 is substituted at R3 and R4 with chlorine groups. The phenyl ring of RTI-111 is attached directly to its tropane ring while in cocaine a carboxylate group bridges the two rings.
Toxicity
The toxicity and long-term health effects of recreational dichloropane use has not been studied in any scientific context and the exact toxic dosage is unknown. This is because dichloropane has very little history of human usage. In terms of neurotoxicity (as defined by the damage or death of cells in the brain in response to over-excitation or reactive oxidation caused by drugs), it is reasonable to assume that like other stimulants which work principally through reuptake inhibition (e.g. cocaine), dichloropane should not exhibit these effects unlike certain other substances such as methamphetamine, which have suspected mechanisms of direct neurotoxicity. The extended use or abuse of dichloropane, however, is likely to cause both short and down-term down regulation of the receptors of the major neurotransmitter (monoamine) systems it interacts with. However, this still remains a subject of active inquiry.
Due to its structural similarity to cocaine, it is worth noting that the most potentially harmful physical effects of dichloropane could not be neurological but cardiovascular. For example, severe cardiac adverse events, particularly sudden cardiac death, become a serious risk at high doses for cocaine due to cocaine’s blocking effect on cardiac sodium channels, and it is possible that dichloropane may share this risk despite not having topical anesthetic activity. Moreover, long-term cocaine usage may result in Cocaine-Related Cardiomyopathy. It is as of yet unknown whether dichloropane presents similar risks, but it is reasonable to assume that it might, and thus should be approached with additional caution.
It is suspected that regular dichloropane insufflation can have extremely adverse effects on one’s nostrils, nose and nasal cavities. These include a loss of the sense of smell, nosebleeds, difficulty swallowing, hoarseness, or a chronically runny nose.
Anecdotal evidence from people who have tried dichloropane within the community suggest that there do not seem to be any negative health effects attributed to simply trying this substance at low to moderate doses by itself and using it sparingly (but nothing can be completely guaranteed).
It is strongly recommended that one use harm reduction practices when using this substance.
Tolerance
As with other stimulants, the chronic use of dichloropane can be considered to have the potential to be moderately addictive with a high potential for abuse, though perhaps less so than that of cocaine, and is thus capable of causing psychological dependence among certain users. When addiction has developed, cravings and withdrawal effects may occur if a person suddenly stops their usage.
Tolerance to many of the effects of dichloropane develops with prolonged and repeated use. This results in users having to administer increasingly large doses to achieve the same effects. After that, it takes about 2 – 4 days for the tolerance to be reduced to half and 1 – 1.5 weeks to be back at baseline (in the absence of further consumption). Dichloropane likely presents cross-tolerance with all dopaminergic stimulants, meaning that after the consumption of dichloropane all stimulants will have a reduced effect.
Withdrawal symptoms
It is possible that after taking dichloropane on a regular or extended basis, some users will become addicted like they would to cocaine. When the drug is discontinued immediately, the user will experience what has come to be known as a “crash” along with a number of other withdrawal symptoms including paranoia, depression, anxiety, itching, mood swings, irritability, fatigue, insomnia, an intense craving for more of the drug, and, in some cases, nausea and vomiting. Some cocaine users also report having similar symptoms to schizophrenic patients and feel that their mind is scattered or incoherent. Some users also report a feeling of a crawling sensation on the skin also known as “coke bugs”.
These symptoms can last for weeks or, in some cases, months. Even after most withdrawal symptoms dissipate most users feel the need to continue using the drug; this feeling can last for years and may peak during times of stress.
Psychosis
Due to its very brief history of human usage, little is known about dichloropane’s ability to induce psychosis, although it is reasonable to assume it presents similar risks to that of cocaine and other dopaminergic stimulants when abused, typically for extended durations, in high doses and or for prolonged periods of time.
| amount | 1 Gram, 3 Grams, 5 Grams, 10 Grams, 25 Grams |
|---|
2 reviews for Dichloropane crystal rocks
Only logged in customers who have purchased this product may leave a review.
Related products


Stimulant
€10.95


Stimulant
€13.95


Stimulant
€10.95


Stimulant
€13.95


Entactogens
€11.95


Stimulant
€13.95


Entactogens
€11.95


Stimulant
€13.95
KobusL45 –
i should find this shop earleir! sick stuff
AndresK25 –
Next level quality! My new fav vendor!